
Patient
HCP
Contact
EN
Menu
Patient
HCP

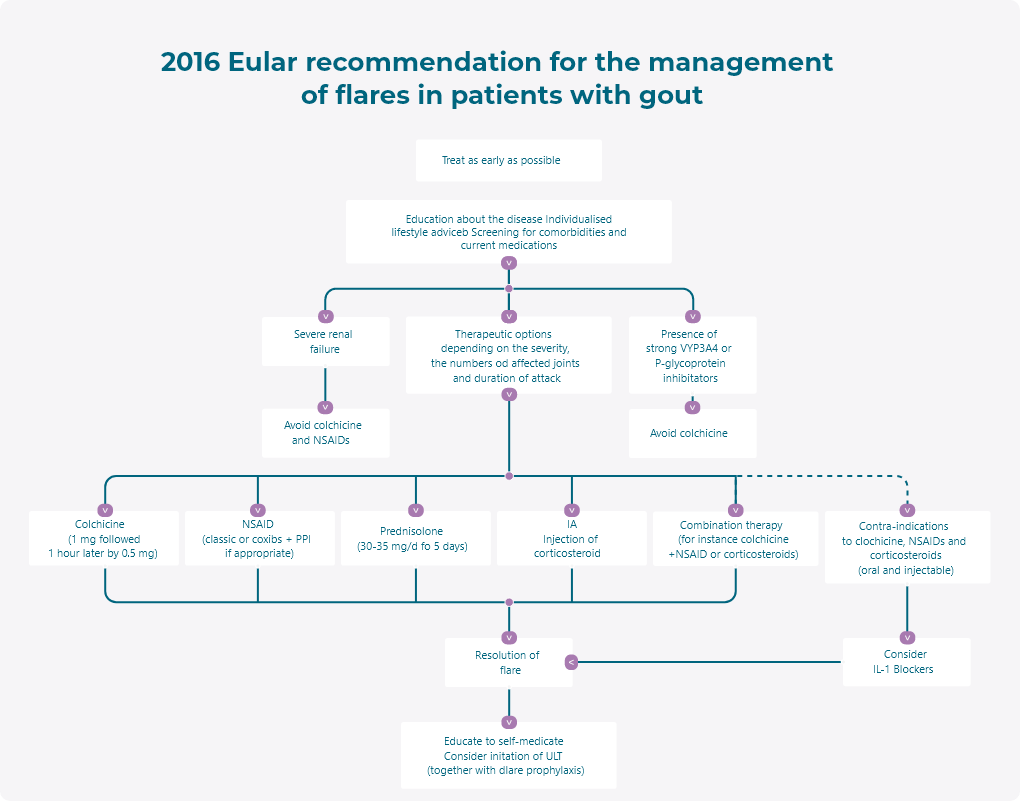
2020 American College of Rheumatology Guideline for the Management of Gout strongly recommend to use colchicine for gout flares management and for gout flares prophylaxis14
Using colchicine, NSAIDs, or glucocorticoids (oral, intraarticular, or intramuscular) as appropriate first- line therapy for gout flares over IL-1 inhibitors or adrenocorticotropic hormone (ACTH) is strongly recommended for patients experiencing a gout flare.
Given similar efficacy and a lower risk of adverse effects, low-dose colchicine over high-dose colchicine is strongly recommended when colchicine is the chosen agent.
For colchicine specifically, the FDA-approved dosing should be followed (1.2 mg immediately followed by 0.6 mg an hour later with ongoing anti-inflammatory therapy until the flare resolves).
Recommendations for choice of initial urate-lowering therapy (ULT) in patients with gout*
| Strongly recommend: |
PICO question |
Certainty of evidence |
|---|---|---|
| For patients experiencing a gout flare, we strongly recommend using oral colchicine, NSAIDs, or glucocorticoids (oral, intraarticular, or intramuscular) as appropriate first-line therapy for gout flares over IL-1 inhibitors or ACTH (the choice of colchicine, NSAIDs, or glucocorticoids should be made based on patient factors and preferences. When colchicine is the chosen agent, we strongly recommended low-dose colchicine over high-dose colchicine given is similar efficacy and fewer adverse effects. | 32 | High |
*PICO = population, intervetion, comparator, outcomes
NSAIDs = nonsteroidal antiimflammatory drugs
IL-1 = interleukin-1
ACTH = adrenocorticotropic hormone
High quality of evidence from network meta-analyses supporting canakinumab, which has superior mean pain score reduction and mean day-2 joint tenderness reduction. However, the Voting Panel raised concern that the comparator was weak (triamcinolone 40 mg) and that costissues significantly favor other agents.
Administering concomitant anti-inflammatory prophylaxis therapy (e.g., colchicine, nonsteroidal anti-inflammatory drugs NSAIDs, prednisone/ prednisolone) over no anti-inflammatory prophylaxis therapy is strongly recommended.
Based on 8 RCTs and 2 observational studies, there is moderate certainty of evidence to support the strong recommendations to use anti-inflammatory prophylaxis therapy when initiating urate-lowering therapy (ULT). Continuation of prophylaxis for at least 3–6 months after ULT initiation was recommended because shorter durations were associated with flares upon cessation of prophylaxis. After cessation, monitoring for flare activity and continuation of anti-inflammatory treatment as needed if the patient continues to experience flares was recommended.
| Strongly recommended: |
PICO question |
Certainty of evidence |
|---|---|---|
| We strongly recommend initiating concomitant antiinflammatory prophylaxis therapy (e.g. colchicine, NSAIDs, prednisone/prednisolone) over no antiinflammatory prophylaxis. The choice of specific antiinflammatory prophylaxis should be based upon patient factors. | 9 | Moderate |
| We strongly recommend continuing prophylaxis for 3-6 month rather than <3 months, with ongoing evaluation and continued prophylaxis as needed if the patient continues to experience flares. | 9 | Moderate |
*PICO = population, intervetion, comparator, outcomes
CKD = chronic kidney disease
NSAIDs = nonsteroidal antiinflammantory drugs
Moderate evidence is in support of the efficacy of pegoticase, but due to cost, safety concerns, and favorable benefit-to-harm ratios of other untried treatment options, the recommendation is against using pegloticase as first-line agent.
Learn more about the 2020 American College of Rheumatology Guideline for the Management of Gout
Click here
Pharmaselect International Beteiligungs GmbH
e-mail: office@pharmaselect.com
Phone: +43 1 786 03 86-0
COLGN-638-01-2412-05



