
Patient
HCP
Contact
EN
Menu
Patient
HCP

The common problem in gout therapy is, that all drugs used might cause severe side effects
Many patients with gout have comorbidities
Therefore, the treatment concept needs to carefully balance the efficacy and the risks
NSAIDS are available in over-the-counter dosing as ibuprofen and naproxen sodium, as well as more-powerful prescription NSAIDs such as indomethacin or celecoxib. Many patients with gout have contraindications to NSAIDs (e.g. hypertension, chronic kidney disease, gastropathy).
A major concern with NSAIDs is their toxicity on the gastronintestinal tract. NSAIDs use is associated with an increased risk of gastrointestinal bleeding and may have cardiovascular toxity.
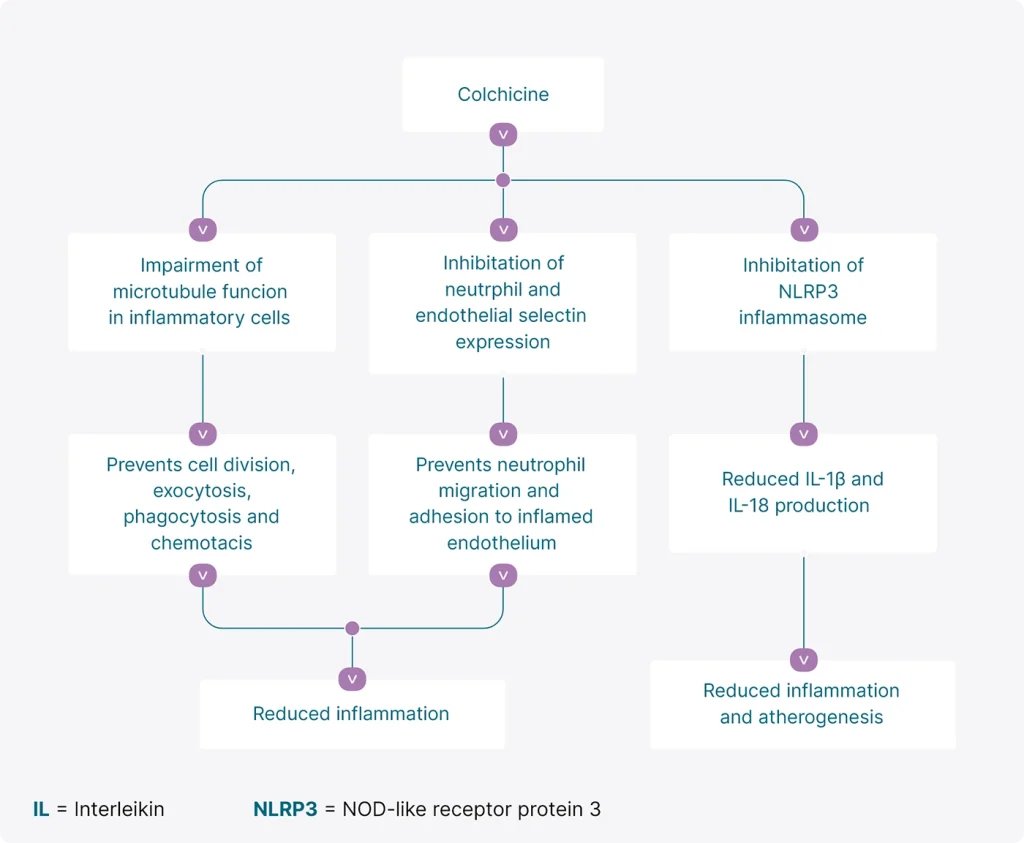
Usually most effective for gout treatment when taken within the first 12 hours of an acute flare. For the first 2 days of treatment co-therapy with NSAIDs can be considered to compensate the delayed onset of pain reduction.
Colchicine dosing schedule is to take 1.2 mg immediately, followed by 0.6 mg an hour later, with ongoing antiinflammatory therapy until the flare resolves.
The drug’s effectiveness may be offset, however, by side effects such as nausea, vomiting and diarrhea, especially in high and frequent dosing. Inappropriate dosing of colchicine occurred frequently and was related to toxicity and death.
Cortisone can be taken orally or injected and quickly suppresses the inflammation of an acute gout flare.
It is important to note that gout flares often occur when a patient first starts taking medications to lower uric acid levels. Patients can help prevent flares when starting these medications by also taking low-dose colchicine or NSAIDs.

Learn more about
colchicine
Pharmaselect International Beteiligungs GmbH
e-mail: office@pharmaselect.com
Phone: +43 1 786 03 86-0
COLGN-638-01-2412-05



